
New York FACE Report: Two Construction Workers Fatally Crushed when Cement Formwork Collapsed
-
Fatality Assessment and Control Evaluation (FACE) Program Reports
The National Institute for Occupational Safety and Health’s (NIOSH) Fatality Assessment and Control Evaluation (FACE) Program and State FACE Programs study fatal workplace injuries and prepare reports with recommendations to prevent similar injuries. The following are links to all of the items in this collection:
Documents
- Kentucky FACE Report: Commercial Roofer Falls 30 Feet Through a Skylight While Installing Roof Insulation
- Fatal Occupational Injuries in Massachusetts 2008-2013
- Fatality Assessment & Control Evaluation (FACE) Program
- Washington FACE Report: Glazier Foreman Falls From Stepladder
- Preventing Construction Falls Toolkit
- Hazard Alert: Pedestrian Workers Killed by Forklifts
- Keep Employees in Motor Vehicles Safe
- New York FACE Brochure
- Washington FACE Report: Construction Laborer Falls When Ladder Breaks
- Washington FACE Report: Pipelayer Dies when Trench Wall Collapses
- Washington FACE Report: Carpenter Falls 60 Feet from Bridge Concrete Form
- Washington FACE Report: Foreman and Laborer Fall when Aerial Lift Struck by Vehicle
- Washington FACE Report: Framer Falls 18 Feet while Sheathing Roof
- New York FACE Report: Mechanic Electrocuted when a Mobile Light Tower Contacted Powerline
- New York FACE Report: Two Construction Workers Fatally Crushed when Cement Formwork Collapsed
- Kentucky FACE Report: Construction Laborer Killed in Trench Collapse while Taking Grade Measurements
- California FACE Report: A Heating, Ventilaton and Air Conditioning (HVAC) Contractor Dies when He Falls through a Skylight
- Massachusetts FACE Report: Carpenter Fatally Injured after Falling from an Extension Ladder
- Massachusetts FACE Report: Laborer Fatally Injured after Falling from a Home under Construction
- Oregon FACE Report: Worker Falls When Ladder Slips
- Michigan FACE Information Sheet: Look for Mobile Equipment Blind Spots
- Oregon FACE Report: Collapsed roof trusses kill carpenter foreman
- Washington FACE Report: Roofer Falls 19 Feet from Roof
- Hazard Alert: Plan. Provide. Train. Prevent Fall Injuries & Deaths
- Kentucky FACE Report: 19-Year-Old Construction Laborer Crushed in Trench Collapse While Laying Sewage Pipe
- Kentucky FACE Report: Construction Flagger Struck and Killed in Two-Lane Highway Work Zone
- Kentucky FACE Report:Temporary Electrician Helper Steps into Unguarded Elevator Shaft and Dies
- Fatality Narrative: Roofing Contractor Falls 25 Feet From Church Roof
- Kentucky FACE Report: Construction Siding Subcontractor Installer Killed when Oversized Scaffolding Platform Destabilized and Telescopic Forklift Overturned
- NIOSH FACE Report - Maintenance Worker Struck by Forklift Carriage—Tennessee
- Kentucky Hazard Alert: Roofing and Construction Workers Killed Due to High Winds
- Poster: Secure it to move it!
- Oregon FACE Report: Crane Operator Killed By Falling Steel Beam
- New Jersey FACE Report: Mechanic Dies After Being Crushed Under Electrical Cabinet
- New Jersey FACE Report: Plant Manager Crushed to Death Under Fallen Pile of Steel Beams
- NIOSH FACE Report: Hispanic worker falls from residential roof
- Oregon FACE Report: Construction worker died after falling 20-25 feet from a pump-jack scaffold
- FACE Fact Sheet: Prevent Construction Falls from Roofs, Ladders, and Scaffolds
- Construction Fatality Narrative: Roofer Falls 18 Feet from Wet House Roof
- Construction Worker Killed when Trench Collapsed, Oregon
- A Tree Trimmer is Electrocuted While Trimming a Palm Tree
- A Tree Feller Dies When Struck By a Tree Limb While Felling a Fire-Damaged Tree
- Concrete Finisher Electrocuted When Bull Float Contacted an Energized Power Line
- Warehouse Worker Crushed by Forks of Laser Guided Vehicle
Summary Statement
On December 2, 2013, a 53-year-old construction laborer and a 50-year-old concrete pump operator suffered fatal crushing injuries when formwork collapsed during concrete placement at a construction site.
December 8, 2017

Photo 1. The site of collapsed form support of buttress
section of aqueduct mockup (photo courtesy of OSHA)
Case Report 13NY080
CASE SUMMARY
On December 2, 2013, a 53-year-old construction laborer (Victim I) and a 50-year-old concrete pump operator (Victim II) suffered fatal crushing injuries when formwork collapsed during concrete placement at a construction site (Photo 1). The concrete piece being constructed was an aqueduct mockup (Figure 1). On the morning of the incident, the workers were pouring concrete to form the left and right buttress sections and the buttress formwork on the right side collapsed. The right buttress formwork had a retaining wall that was composed of a lower vertical face and an upper inclined face (Figure 2). At the time of the incident, Victim I and Victim II were working from a platform abutting the retaining wall. At around 12:30 pm when the freshly poured concrete was approximately 10 feet high, workers heard loud thudding noises as the retaining wall and the work platform collapsed. A 911 call was placed immediately and EMTs arrived at the site within minutes. Victim I was trapped underneath the formwork and pronounced dead on the scene. Victim II was also trapped underneath the formwork but rescued by other workers who used a forklift to lift the formwork to free him. Victim II died in a hospital nine days later from crushing injuries. Post incident investigations identified several discrepancies between what the formwork design specified and how the formwork was constructed. The formwork deviated from the design specifications in the type, size, and number of anchors to be installed. Pipe braces and hold-down brackets indicated on the drawings were not installed. The formwork did not have adequate capacity to resist the horizontal fluid forces and lacked any mechanism to resist the uplift force on the formwork during concrete placement. The formwork failed due to a combination of mechanisms including formwork uplift followed by wash-out of the wood base platform, vertical drop and collapse of the support wall, and shear/tension failure of the anchoring system.
CONTRIBUTING FACTORS
- Formwork did not have adequate design capacity and mechanisms to resist the loads and forces on the structure during concrete placement.
- Formwork was not constructed according to design specifications.
- Changes made during formwork construction were not approved by the design engineer.
- Formwork was not braced and tied down according to drawings.
- Formwork was not inspected and certified to meet design specifications prior to concrete placement.
- Signs of formwork distress during concrete placement were not adequately evaluated.
- Competent person was not on site during concrete placement.
- Formwork drawings were not available on site.
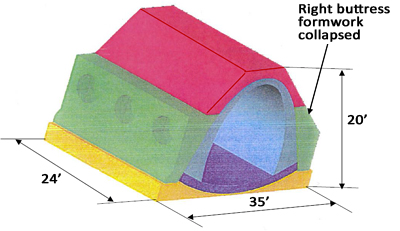
Figure 1. Aqueduct mockup to be constructed in five pours
KEY RECOMMENDATIONS
- Employers should ensure that concrete formwork has adequate designed capacity and mechanisms to resist loads and forces during concrete placement.
- Employers should ensure that concrete formwork is constructed strictly following design specifications.
- Employers should ensure that concrete formwork is braced and tied down adequately to stay in alignment and retain stability.
- Employers should inspect formwork at each stage of construction as well as prior to and during concrete placement to ensure formwork quality.
- Employers should ensure that a competent person is on site during formwork construction and concrete placement.
- Employers should establish and implement a standard operating procedure on how to identify, document, report, and resolve deviations from design on formwork.
- Employers should hold a formwork plan review meeting involving both design and field construction personnel prior to start of formwork construction.
- Employers should conduct a job hazard analysis and provide worker training on risks and hazards associated with formwork construction and concrete placement.
- Employers should keep concrete formwork drawings easily accessible to construction crew.
INTRODUCTION
On December 2, 2013, a 53-year-old male construction laborer (Victim I) and a 50-year-old male concrete pump operator (Victim II) suffered fatal crushing injuries when formwork collapsed during concrete placement at a construction site. The New York State Fatality Assessment and Control Evaluation (NY FACE) staff learned of the incident from news media and initiated an investigation. The NY FACE investigator conducted a site visit and reviewed formwork drawings, incident site photos, concrete work records, and a structural forensic investigation report. The structural forensic investigation was conducted by a firm hired by Victim I’s employer, a civil construction company. The case was discussed with the compliance officers from the Occupational Safety and Health Administration (OSHA) who investigated the incident. The New York City Department of Environmental Protection (NYCDEP) that managed the construction project provided additional information. The NY FACE investigator consulted two professional engineers (PEs) on the causes and mechanisms of the formwork collapse. This report summarizes the findings of the NY FACE investigation.
The civil construction company that employed Victim I had approximately 180 employees including 80 union workers. Victim I was a union member. The civil construction company was the general contractor (GC) for a NYCDEP’s major water project involving renovation of two underground aqueducts. Victim II’s employer, a concrete pumping company, was one of the subcontractors on the project.
Aqueduct renovation included demolition of existing structures and construction of new piping and connection systems. One component of the project was to produce a full-scale aqueduct replica (mockup) which would be used for testing and practicing the connection methods. The mockup was constructed at a secondary work site 15 miles from the main site. The incident happened during construction of the mockup.
INVESTIGATION

Photo 2. Completed buttress formwork on the morning of the incident.
The aqueduct mockup was shaped like an arched tunnel. It was approximately 20 feet tall, 35 feet wide, and 24 feet long (Figure 1). The mockup was to be constructed in five concrete pours: Pour I - rock simulation slab (shown in yellow); Pour II – aqueduct slab (shown in purple); Pour III - aqueduct wall (shown in blue); Pour IV - aqueduct buttress section including left and right buttresses (shown in green); and Pour V - aqueduct crown encasement (shown in red).
The rock slab (Pour I), aqueduct slab (Pour II), and aqueduct wall (Pour III) were poured and cured prior to the incident. The incident occurred during pour IV when the buttress formwork on the right side collapsed.
The right buttress formwork was composed of a retaining wall along the length of the mockup and a side panel at each end (Photo 2). The three-sided enclosure was attached and secured to the aqueduct wall. The retaining wall and side panels were built on top of the rock simulation slab. A work platform was constructed abutting the retaining wall.
The retaining wall had a lower vertical face and an upper inclined face with a 42-degree slope (Figure 2). The vertical panel was set on the cured rock simulation slab that was approximately 3’ 2 5 ⁄8” above the ground. Both faces, made of plywood panels with metal framing and timbers, were held up and supported by tie rods that were inserted into the existing concrete structure and secured by anchors, nuts, and bolts. The drawings indicated that wood sill plates and hold-down brackets were to be installed on the base of the retaining wall and that the retaining wall should be braced by pipe braces.
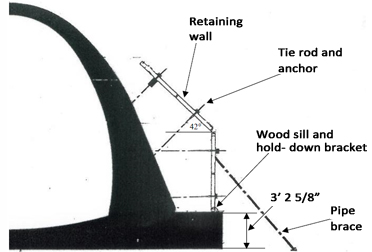
Figure 2. Retaining wall on the cured concrete structure
On the day of the incident, four workers including Victim I arrived at the mockup site at around 7 a.m. They were to complete the final stage of formwork erection and assist with concrete placement. Two foremen arrived 45 minutes later. They brought two concrete vibrators and informed the crew that the concrete trucks would start arriving around 9 a.m. After discussing the day’s work with the crew, both foremen left the site and returned to the main office at around 8:30 a.m. The crew continued working on the formwork until 8:50 a.m. when the first concrete truck arrived. Victim II arrived sometime before 8:50 a.m. There were also two NYCDEP inspectors at the site.
The first truck started pouring at around 9 a.m. Between 9 a.m. and 12 p.m. seven trucks each carrying 10 cubic yards of concrete poured the buttress sections on either side alternately to keep the mockup in balance. The pour rate was approximately two to three feet (in thickness or height) per hour. Working from the platform, the crew poured concrete and operated two cement vibrators.
At around 10:20 a.m. when the fourth truck was pouring the left side, a worker felt a movement in the formwork. He informed the lead person of the group who had also heard the noise. The lead person stopped the pouring at the left side. The rest of the load was placed in the right-side buttress. The lead person called the foreman in the main office and asked if the foreman could get the formwork drawings and check whether the formwork was assembled correctly. There were no formwork drawings kept at the mockup site. The foreman said that he would look for the drawings in the main office.
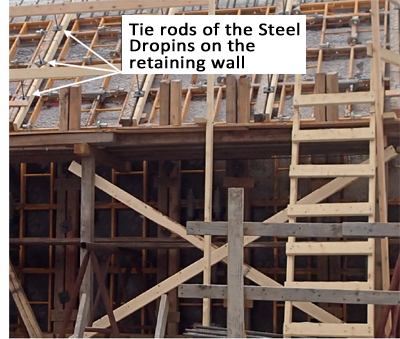
Photo 3. There were approximately 45 anchors on the support
wall in six rows: three restraining the lower vertical face and
three restraining the upper inclined face (Photo courtesy of
NYSDEP).
Meanwhile the crew found a loose nut on the left-side formwork and tightened it. The crew installed a diagonal lumber brace in the middle of the left retaining wall to strengthen it. The lead person called the foreman back informing him that the problem was solved and everything was going well.
The seventh concrete truck arrived at 11:21 a.m. The lead person called the foreman again at 11:42 a.m. and notified him that the job was going well except that they were going to run out of concrete. The foreman ordered another 10 cubic yards of concrete.
The seventh truck started pouring the right buttress at 11:58 a.m. One worker was on top of the formwork guiding the pump hose and operating the vibrator. Victim I was in the middle section of the platform assisting pouring. Victim II was also on the platform operating the pump hose. Two workers including the lead person were on the ground.
Another foot of concrete (in height) was poured when the worker who was operating the vibrator noticed a tie rod sliding out of the formwork. The pouring stopped. The lead person got on the platform to look at it. He tightened the rod and concrete pouring resumed.
At around 12:30 p.m. when the freshly poured concrete was approximately ten feet high, workers heard loud thudding noises as the retaining wall collapsed along with the work platform. A 911 call was placed immediately and EMTs arrived at the site within minutes. Victim I was trapped and crushed underneath the formwork and pronounced dead at the scene. Victim II was also trapped underneath the formwork but rescued by other workers who used a forklift to lift the formwork to free him. Victim II died from the crushing injuries in a hospital nine days after the incident. The worker who was on top of the formwork was partially trapped underneath the collapsed structure. He was pulled out by co-workers immediately. He survived with multiple injuries including a broken shoulder, laceration to the head, and contusions.
Post incident investigations identified several discrepancies between what the formwork design specified and how the formwork was constructed. The original design (shop drawings) specified an adhesive anchoring system (HIT-HY 150 Max Adhesive Anchoring System). The adhesive anchoring system mainly consisted of a threaded tie rod and a fast curing adhesive. The tie rod was to be inserted into a properly sized hole in the concrete that was filled with adhesive. The adhesive would bond the rod with the concrete. The design specified installing fifty-two ⅝” diameter rods in four rows with 13 anchors per row. Two rows on the vertical face, and two on the upper inclined face. The allowable tension capacity of each adhesive anchor was 8,410 lb.
While assembling the formwork at the site, a mechanical anchor system was used instead due to the concern that the adhesive might not work well in low temperatures. The mechanical anchor system used was Steel Dropin manufactured by Powers Fasteners, Inc. The anchor was ½” in diameter and 2” in length. It was held in the concrete by pressure and friction. The Steel Dropin had an allowable capacity of 1,440 lb. that was less than one fifth (17%) of the adhesive anchoring system. There were no written records indicating that the change was reviewed and approved by the design engineer.
The total number of the Steel Dropins installed and their exact locations on the retaining wall were not available. The photo that was taken on the morning of the incident showed approximately 45 anchors in six rows; three restraining the vertical face and three restraining the inclined face. Table 1 summarizes how the anchoring systems on the support wall deviated from the design specifications.
| Original Design Specification | As-Built Conditions | |
| Type of Anchoring System | Adhesive anchor | Mechanical anchor |
| Number of anchors | 52 | 45 |
| Anchor rod diameter | 5/8" | 1/2" |
| Allowable tension capacity per anchor (lb.) | 8,410 | 1,440 |
The drawings indicated five pipe braces (four feet apart) in lengths between 3.6 and 4.8 meters (between 11.8 and 15.75 feet) to be installed at approximate 45° (degree) angles against the vertical formwork face and seated in pipe brace shoes (Figure 2). These pipe braces were to provide additional support to counter the horizontal fluid forces. None of the braces was installed.
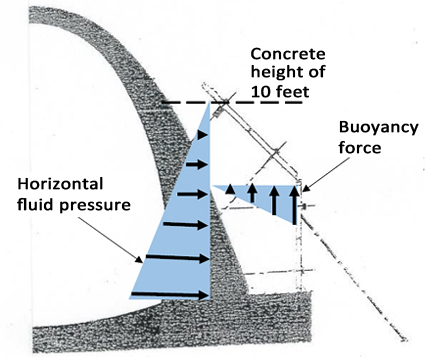
Figure 3. Illustration of direction and distribution of forces on the
formwork at the time of collapse.
The forensic investigators concluded that the primary failure method was anchor failure at the bottom row which caused progressive anchor and formwork failure. Their conclusion was based on two assumptions: 1) there were 24 anchors installed on the formwork; and 2) that the only force on the formwork at the time of structural failure was the horizontal fluid pressure exerted by the fresh concrete. However, the evidence showed otherwise. The anchors in the bottom row did not all fail. In fact, the only anchors on the whole retaining wall that stayed in the concrete were the five anchors in the bottom row. There were approximately 45 anchors on the formwork, far more than 24 (Photo 3). The forensic investigators declined to provide an explanation of their assessment.
To find out whether there were additional contributing factors to the structural failure, the NY FACE investigator consulted with two PEs of a civil engineering company. The PEs established a twodimensional finite element model of the formwork, subjected the model to the forces and loads that the formwork was subjected to during the concrete placement, assessed the likely behavior of the formwork based on its unique geometry, identified an additional force on the formwork, and proposed the likely causes and failure mechanisms of the formwork collapse.
At the time of the incident, there were approximately 10 feet (in height) of fresh concrete that weighed approximately 145 to 150 pounds per cubic foot placed in the formwork. The formwork was subjected to not only the horizontal fluid pressure but also a buoyancy force generated by the upper inclined wall (Figure 3). When fresh concrete pressed against the inclined face, it generated an uplift force that would move the formwork upward. The only mechanism on the retaining wall that might have had some capacity to resist uplift was the hold-down brackets. The design did not provide any specifications on the type, size, and installation requirement of the hold-down brackets and the holddown brackets were never installed.
Since the exact number and locations of the anchors on the retaining wall cannot be verified and confirmed, the tension force on each anchor cannot be calculated. However, comparison of allowable tension capacity of the two types of anchors, and the number of anchors on the drawings and on the actual formwork suggested that the capacity of the mechanical anchoring system was not sufficient. The PEs concluded that the as-built formwork was not adequate to resist the horizontal fluid concrete forces and lacked any mechanism to resist the uplift force on the formwork.
The formwork failed due to a combination of mechanisms including formwork uplift followed by wash-out of the wood base platform, vertical drop and collapse of the retaining wall, and tension failure of the anchoring system. The failure likely started with a release of fresh concrete at the base of the formwork, as evidenced by the work platform being thrust a distance away from the concrete wall significantly greater than its original height from grade. The release of concrete at the base was likely caused by the uplift of the vertical face due to the buoyancy force.
The retaining wall was then pushed away from the mockup and fell vertically off the slab. There were five anchors near the bottom that remained embedded in the concrete section. These rods remained perpendicular to the concrete section for a short distance and then bent at a sharp, nearly 90° angle downward (photo 4). This suggests a vertical drop in the formwork wall prior to major lateral movement. Tension failure of the anchors was the third and last stage of failure, allowing lateral rotation of the formwork about its base and away from the mockup.
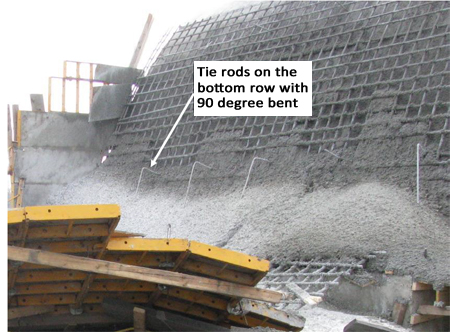
Photo 4. Tie rods that remained on the concrete bent at a nearly 90
degree angle suggesting a vertical drop in the retaining wall during
collapse (photo courtesy of OSHA).
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that concrete formwork has adequate designed capacity and mechanisms to resist loads and forces during concrete placement.
Discussion: Concrete formwork is not only a mold for shaping fresh concrete to the desired shape and size, but is also a structure for supporting “dead” and live loads during formwork construction and concrete placement. The dead loads include the weight of fresh concrete and the weight of formwork itself. The live loads include the weight of workers, equipment, and materials. Unique geometry of the formwork may subject it to additional forces. Employers should ensure that formwork has adequate capacity and mechanisms to withstand the loads and forces applied to the structure.
The formwork in this case did not have adequate capacity and mechanisms by design to resist the forces and prevent the formwork from moving upward. The buoyancy force was generated by the inclined wall face. The only mechanism that might have resisted the buoyancy force was the wood sill plate and hold-down bracket. However, the drawings did not specify the type, size, and installation requirement. Employers should ensure that the drawings have clear specifications on the mechanisms that are critical for preventing formwork failure.
Recommendation #2: Employers should ensure that concrete formwork is constructed strictly following design specifications.
Discussion: A properly designed formwork has the rigidity, stability, and durability necessary to withstand the applied loads. Deviations from the original design not approved by the design engineer can lead to formwork failure causing serious worker injuries and deaths. Employers should ensure that formwork is constructed strictly following original design specifications. If modifications of the original design are needed, the changes must be reviewed and approved by the design engineer.
The construction of the formwork in this case used a different anchoring system that had far lower capacity than the design specification and the change was not approved by the design engineer. This deviation contributed to the formwork collapse, resulting in worker injury and deaths.
Recommendation #3: Employers should ensure that concrete formwork is braced and tied down adequately to stay in alignment and retain stability.
Discussion: Formworks should be braced and tied down to stay in alignment and retain their structural stability. Although braces and tie-down wares are usually not considered as part of the design, they are critical for preventing formwork failure. Employers should ensure that the construction crew receives clear installation specifications from design engineers and braces and ties down the formwork strictly following the design requirement.
The aqueduct drawings in this case indicated five pipe braces to be installed at approximate 45° (degree) angles against the vertical formwork face. These pipe braces were to provide additional support to counter the horizontal fluid forces. None of the braces was installed. The drawings also indicated ¾” wood sill plate to be secured by hold-down brackets at the base of the vertical wall face. The sill plate and hold-down brackets were not installed.
Recommendation #4: Employers should inspect formwork at each stage of construction as well as prior to and during concrete placement to ensure formwork quality.
Discussion: Formwork should be inspected at each stage of construction to ensure that it is constructed per design specifications. Concrete pour has the highest risk for severe injuries and deaths which are mostly associated with catastrophic formwork failures. Before concrete placement begins, formwork must be inspected and signed off on by an engineer or competent person. The final inspection should include braces and tie-down hardware on the formwork. Any discrepancies should be resolved with the design engineer. Unless all discrepancies are resolved, or changes are approved by the design engineer, concrete placement cannot proceed.
Inspection of formwork should continue during concrete placement. If there are signs of formwork movement, or deflection or failure of the anchoring system, pouring should be immediately suspended. Concrete pour should not resume unless the situation is properly evaluated and corrected.
Recommendation #5: Employers should ensure that a competent person is on site during formwork construction and concrete placement.
Discussion: Employers should ensure that a competent person is on site during formwork construction and especially during concrete placement. A competent person is someone who is capable of identifying the risks and hazards associated with formwork construction and concrete placement and has the authority to take corrective measures to eliminate the danger and hazards to workers.
There were signs of problems with the formwork during concrete pouring in this case. A competent person could have suspended the concrete placement prior to the catastrophic formwork failure.
Recommendation #6: Employers should establish and implement a standard operating procedure on how to identify, document, report, and resolve deviations from design on formwork.
Discussion: Employers should establish a standard operating procedure (SOP) on how to identify, document, report, and resolve deviations from design on formwork during construction and concrete placement. The SOP should clearly define the responsibilities of personnel involved, the reporting chain, and the follow up actions to review and ensure that the issue is properly resolved. The SOP should also specify what actions should be taken once a movement or deflection is detected on the formwork during concrete placement. The employers should ensure that all staff involved are familiar with and strictly follow the SOP.
Recommendation #7: Employers should hold a formwork plan review meeting involving both design and field construction personnel prior to start of formwork construction.
Discussion: A formwork plan review meeting should be held in the project planning stage. The meeting should include both design engineers and field construction personnel such as the competent person, supervisors, and lead persons. The design engineers can help the construction staff understand the high-risk features on the formwork as well as the critical mechanisms to prevent structural failure. All sides can learn and review the SOP on how to deal with deviations from design in construction. With a better understanding of critical safety features on the formwork, the importance of following design drawings, and the consequences of not following the design specifications, the field crew would be less likely to take short cuts or modify the structure without consulting the designing engineer.
Recommendation #8: Employers should conduct a job hazard analysis and provide worker training on risks and hazards associated with formwork construction and concrete placement.
Discussion: Workers can be exposed to multiple hazards such as fall, crushing, or struck-by injuries during formwork construction and concrete placement. A job hazard analysis can identify the specific hazards and help employers to develop specific prevention measures and training materials.
Worker safety during concrete work is closely tied to the quality of the formwork. Deviations from design specifications not approved by design engineers can lead to catastrophic structural failure and worker deaths. Employers should provide training to field supervisors, lead persons, and workers on the importance of building formwork according to the design, as well as and the consequences of not following the design. The training may include:
a. high risk features of the formwork
b. critical mechanisms on the formwork to retain structural stability and prevent failure
c. the importance of following design specifications
d. the importance of following the manufacturer’s requirement to install anchors and other parts
e. standard operating procedure on documenting and reporting deviations from design on the formwork.
Recommendation #9: Employers should keep concrete formwork drawings easily accessible to the construction crew.
Discussion: The formwork drawings in this case were not kept on site. Instead, they were kept at the main working site approximately 15 miles away from the mockup construction site. Concrete formwork drawings should be easily accessible to the construction crew so that they can check and verify whether the formwork structure is constructed according to the drawing specifications.
Keywords: concrete formwork, formwork failure, construction, crushing injury, formwork collapse, concrete placement, inclined support wall, buoyancy force, formwork uplift, aqueduct
ACKNOWLEDGEMENT
Ryan Biggs/Clark Davis Engineering and Surveying, P.C. provided formwork structural analysis.
REFERENCES
- Safety and Health regulations for Construction, Concrete and Masonry Construction. 29CFR. 1926.703. Occupational Safety and Health Administration. United States Department of Labor. Feb 13, 1996. Retrieved February 28, 2017 from https://www.osha.gov/laws-regs/regulations/standardnumber/1926/1926.703
- Use and Re-use of Formwork: Safety Risks and Reliability Assessment. CPWR Small Study Report. Retrieved March 17, 2017 from http://www.cpwr.com/sites/default/files/publications/GambeteseFormworkUseandRe-useFinalReport.pdf
- Prevention formwork failures, Information about preventing formwork failure and concrete collapse during concrete pours. Work Safe Victoria. Retrieved January 21, 2016 from http://www.worksafe.vic.gov.au/__data/print_to_pdf.php?url=http://www.worksafe.vic.gov.au/forms-and-publications/forms-and-publications/preventing-floor-collapse2/_nocache%3FSQ_DESIGN_NAME=blank%26SQ_PAINT_LAYOUT_NAME=pdf
- Concrete Formwork Loads and Pressure Calculations. The Constructor-Civil Engineering Home. Retrieved March 23, 2017 from https://theconstructor.org/building/concrete-formwork-loads-pressure-calculations/14521/
Andrew M. Cuomo
Governor
Howard A. Zucker, M.D., J.D.
Commissioner
Sally Dreslin, M.S., R.N.
Executive Deputy Commissioner
The New York State Fatality Assessment and Control Evaluation (NY FACE) program is funded by the National Institute for Occupational Safety and Health and administered by the New York State Department of Health. NY FACE is a research program designed to study the causes of workplace fatalities and develop practical and effective prevention measures. NY FACE investigators evaluate information from multiple sources and provide recommendations for prevention in summary reports. These recommendations are distributed to employers, workers, and other organizations interested in promoting workplace safety. The NY FACE does not determine fault or legal liability associated with a fatal incident. Names of employers, victims and/or witnesses are not included in written investigative reports or other databases to protect the confidentiality of those who voluntarily participate in the program.
Additional information regarding the NY FACE program can be obtained from:
New York State Department of Health FACE Program
Bureau of Occupational Health and Injury Prevention
Corning Tower, Room 1325
Empire State Plaza
Albany, NY 12237
866-807-2130
518-402-7900
boh@health.ny.gov
https://www.health.ny.gov/environmental/investigations/face/
